Forum of people who use drugs (PWUD) Kazakhstan
Forum of people who use drugs (PWUD) Kazakhstan is a civil forum, a community of people who use drugs and their supporters, activists and experts in the field of drug policy, who areunited by common goals and interests. The mission of the Forum is to mobilize people who use drugs for joint action and structural changes in Kazakhstan drug policy in accordance with the interests and needs of the PWUD, based on standards of human rights and fundamental freedoms, as well as standards of medical care and social support for the PWUD recommended by the World Health Organization (WHO). Currently, the Forum has 21 people - these are activists from 7 regions of Kazakhstan.
How did you decide to focus on the topic of peer-to-peer consultants? Why is this topic relevant in Kazakhstan?
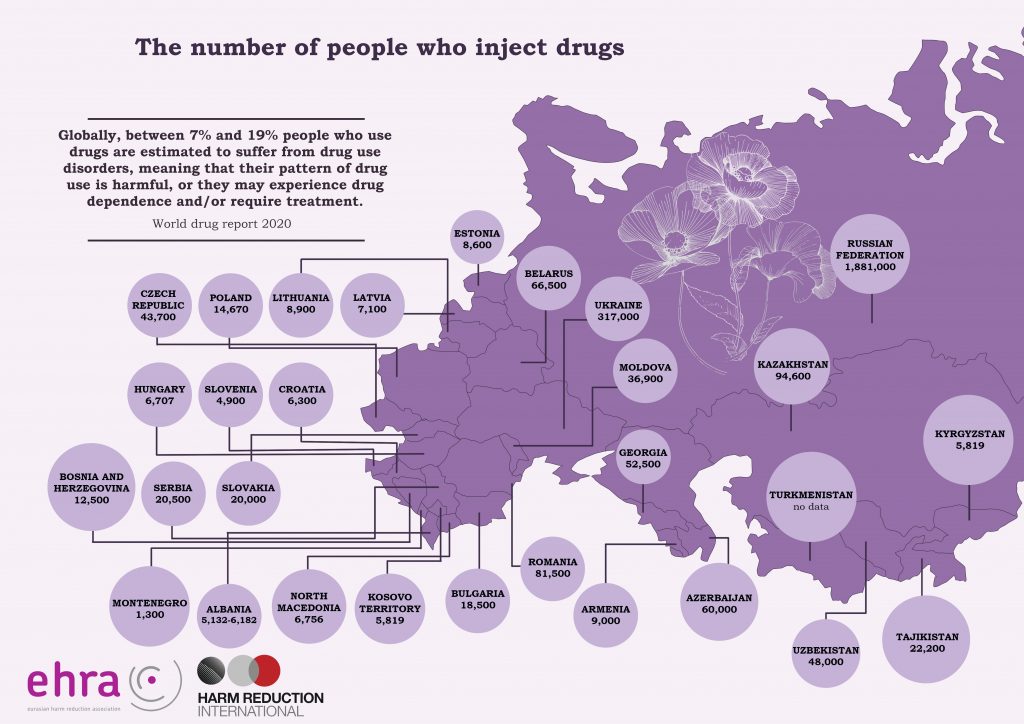
Starting from 2014, there is a growth of the NPS market in Kazakhstan. Compared to other Central Asia countries, Kazakhstan has the highest number of NPS reported. More about NPSs in Kazakhstan can be found in the report “New psychoactive substance use in the Republic of Kazakhstan: Research results.
Most harm reduction services in Kazakhstan are oriented at opiate users, although the drug scene is changing: the opiate market is slowly disappearing. As a result, fewer people with opioid dependence are registered each year, while NPS appear on the market. With the changing drug scene, outreach work to support people with opioid dependence has become less effective. Activists from the community of PWUD in their 30s are those who have been clients of harm reduction programs and started to use synthetics. Young people aged 12-30 who have never tried opiates now snort and smoke, prefer to smoke NPS, and mix substances with tramadol and stimulants (part of this group are directly related to darknet advertising, distribution, etc.) and then switch to injecting.
No one in Kazakhstan has previously implemented projects aimed at supporting people who use NPS in the online platforms. This topic was also new for us, but we already had little experience in consulting people who use NPS on social networks (Telegram) as volunteers in darknet. The project became an opportunity for us to do it more professionally and qualitatively with the ability to pilot its results to all interested parties to expand the package of services and subsequent implementation of the online consultation componentfor PWUD at the country level.
What is an online peer-to-peer consultation? How does it work? Tell us more about how you do these consultations.
Online peer consultation is the work in a variety of online formats:
-publications, posts with information on safe drug use that we collect and prepare ourselves (types of NPS, characteristics, effects, consequences of use; poly-drug use);
– thematic photos, GIFs, videos;
– trip-reports (when people share their personals stories related to substance use). It is a great material, and it is always interesting to read it. It can also inform people about the negative consequences of using a substance they are trying for the first time;
– peer-to-peer psychological support is a support without shaming or blaming person, with the opportunity to share personal experience;
– referral to specialized professionals (psychologist, addictologist, infectious diseases specialist);
– online lawyer of the Forum of PWUD Kazakhstan;
– consultations on HIV/ AIDS, hepatitis, STIs;
– HIV testing;
– consultations on access to social and medical services;
– informing about the activities of PWUD Kazakhstan Forum, ENPUD, EHRA – organizations that support PWUD in the region;
– invitations to participate in open discussions, online webinars for PWUD;
– invitation to participate in the campaigns with the international community of PWUD;
– referrals, accompanying, personal face-to-face meetings;
– thematic surveys (HIV, hepatitis, on the content of the channel).
What problems did you face, when you started to provide online consultations?
The difficulties that we faced, when we started to provide online consultations are the distrust and closeness of users of Telegram channels. Even now for people who use NPS it is difficult to trust and understand that there are people in Kazakhstan, who are providing harm reduction services, who are openly speaking at one’s own risk about themselves, their experience of drug use, and support you psychologically. The difficulty is in the communication and personal contacts because some help implies private meetings, for example, social accompanying, and this kind of activity is excluded by the rules of Telegram users.
Only few people contacted the project lawyer. According to the results of a face-to-face survey, we realized that people simply do not trust such a service. It is something new for them, and it is difficult for people who use drugs to talk to a person with a legal background about personal use or to solve similar issues.
Please share your achievements in this small grant.
One of the most significant achievements of the project was the launch of three Telegram channels, where around 400 people subscribed. These are people who receive information on harm reduction,, what to do in case of overdose, receiving social, medical and legal assistance. The most important thing is that in case of any problems they know where and whom they can ask for help or advice.The audience also participated in two campaigns: on August 31 in the World Overdose Awareness Day and Support Don’t Punish (World Drug Day).
Users have also noted the value and necessity of the publications in the channels, as well as the existence of such content and the service in general.
Medical workers, the expert community, GFATM, representatives of international organizations in Kazakhstan also share this opinion. At the moment the information about piloting the service online – consultations were presented on two platforms, where all interested state parties (Kazakh scientific center of dermatology and infectious diseases, Republican Scientific and practical center of mental health,, CCM, etc.) and international organizations (UNAIDS, UNODC, GFATM, etc.) were present.
We mastered the skills of running Telegram channels, learned how to work through bot-support, and learned a lot of useful information while compiling and selecting material for publications. We gained experience in creating promotional materials focused on the needs of the community of people who use NPS.
Consultations and support for people who use NPS is also a new experience for us, and we are pleased with the result we got. Acceptance and trust is the most important thing.
Now that the project is over, people from other regions have joined the channels, and one of them asked us for support. Our consultant helped us to create a channel, and now we have another additional resource where we can talk about harm reduction.



Your recommendations for donors/government to promote this approach. What are the next steps?
- The Forum has planned further steps to improve and expand online services. For example, attracting funds to provide services of addictologist, psychologist, distribution of informational material on harm reduction. We submitted one grant application, now we are waiting for the results.
-Technical support (laptops, software to work with video, create promotional materials, etc.) is needed for the implementation of such projects;
– educational pieces of training, offline seminars;
– capacity building of the team, psychological support for online consultants;
– development of a security plan with the involvement of specialists as NPS attracts the attention of the police;
– organizational and personal security;
– IT security
– contacts of friendly lawyers, psychologists
- There is a need for intensive outreach work with NPS users. Access to prevention programs for new people will become more effective if information about services will be disseminated through Internet resources, pharmacies, mobile sites, nightclubs.
- It is not known precisely how many people are members of groups where sexual contacts are connected with the use of NPS. It is worth noting that offers of substance use in exchange for sexual services for girls are common in Тelegram channels. This type of “leisure” is popular.
The risks of HIV infection and other STIs are increasing significantly. Therefore, it is necessary to develop services aimed at the sexual and reproductive health of women who use synthetic substances, involving medical specialists (gynecologists, dermatovenerologists). It is essential to educate project consultants on specific topics of counseling, to provide lubricants, female condoms, etc. in larger quantities.
- Creation of an international online platform for communication on harm reduction for NPS users:
– Implementation of projects towards online consultation on NPS (sharing experience)
– Mobilization and support for people working with NPS issues
– trainings
– development of new concepts, plans, materials on NPS